|
Case Series
Cryptococcus in the absence of immunosuppression: Diagnostic and therapeutic challenges
1 Department of Infectious Disease, The University of North Carolina at Chapel Hill, Chapel Hill, North Carolina, USA
2 Department of Immunology, The University of North Carolina at Chapel Hill, Chapel Hill, North Carolina, USA
Address correspondence to:
Salma Gayed
Department of Medicine, Division of Infectious Disease, The University of North Carolina at Chapel Hill, 101 Manning Drive, Chapel Hill, North Carolina 27514,
USA
Message to Corresponding Author
Article ID: 100021Z16SG2026
Access full text article on other devices

Access PDF of article on other devices


How to cite this article
Gayed S, Schworer S, Yalin E, Stromberg J, Herce M. Cryptococcus in the absence of immunosuppression: Diagnostic and therapeutic challenges. J Case Rep Images Infect Dis 2026;9(1):13–18.ABSTRACT
Invasive cryptococcal infections, particularly those caused by Cryptococcus neoformans, are significant contributors to morbidity and mortality among immunocompromised patients, especially individuals living with human immunodeficiency virus/acquired immunodeficiency syndrome (HIV/AIDS). Recognized as a critical fungal pathogen by the WHO in 2022, the increasing prevalence of such infections raises concerns, particularly as case reports emerge detailing instances in seemingly immunocompetent individuals. Here we report two cases, one in which the host had no known immunocompromising condition at time of diagnosis, and the other in which invasive infection was found without clear evidence of pulmonary or neurological involvement. We discuss the evolving epidemiology and diverse manifestations of invasive cryptococcal infections, and emerging associations with conditions that may predispose to infection in the seemingly immunocompetent host. These cases highlight disseminated cryptococcosis in patients without traditional severe immunosuppression, emphasizing the need for high clinical suspicion.
Keywords: Cryptococcus neoformans, Diffuse large B-cell lymphoma, Disseminated cryptococcosis, NASH cirrhosis, Non-HIV immunosuppression
Introduction
Invasive cryptococcal infections in immunocompetent individuals have been thought to be a rare occurrence, and most published case studies highlight possible risk factors, including undiagnosed immunodeficiencies, malignancies, chronic lung disease, and host genetics [1]. However, the prevalence of cryptococcus in individuals without known causes of immunosuppression is higher than conventionally thought, representing 20% of reported cases in one multicenter cohort study of 306 patients from 1990 to 1996 [2]. Additionally, common conditions such as diabetes, NASH cirrhosis, or alcohol use may represent subtle ongoing immunosuppression that predisposes to infection. Traditionally, pulmonary and neurological involvement were felt to be the hallmarks of invasive infection. But clinical presentations can vary widely, and the underlying pathophysiology is not always well understood, which can create diagnostic and therapeutic challenges.
Case Report
Case 1: Disseminated Cryptococcal Infection
A male patient in his seventies presented to the emergency department with altered mental status for a week prior to admission, weakness, and recurrent falls without loss of consciousness. Although the patient did not have classical immunosuppression, he did have a history of uncontrolled diabetes, NASH cirrhosis (complicated by esophageal varices and a history of trans jugular intrahepatic portosystemic shunt in 2016), and a history of diffuse large B cell lymphoma, diagnosed 2018 and in remission (with a history of receiving chemotherapy several years prior, but details not known at time of admission), which likely contributed to altered host defenses. He also had coronary artery disease, atrial fibrillation, asthma, gout, and hypertension. He lived with his family and was a former smoker with a 6-pack year history but quit 26 years ago.
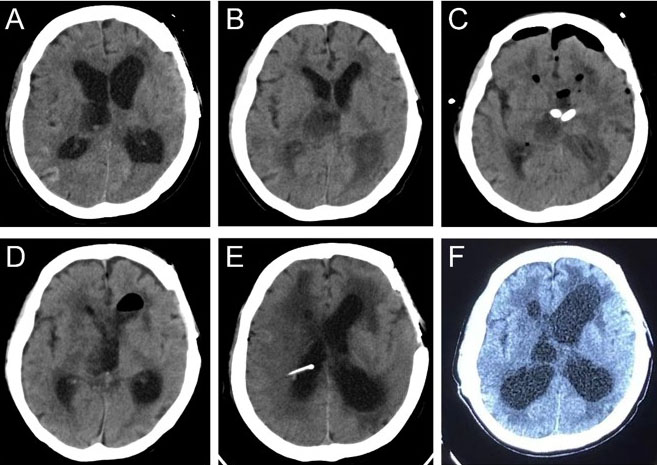
He initially presented to an outside hospital for worsening altered mental status and, in the emergency department (ED), was noted to have a fixed upper gaze and seizure-like activity. A code stroke was deployed, and a head computed tomography (CT) was notable for new left-sided subdural hematoma, thought due to falls at home. He was transferred to our tertiary center for intensive care. He became febrile one week into his hospitalization and remained persistently febrile, prompting the collection of peripheral and central line blood cultures and infectious disease evaluation. His hospital course was further complicated by progressively worsening mental status and generalized jerking movements, prompting anti-epileptic treatment. A repeat CT head revealed bilateral subdural hygromas and an increase in size of the left-sided subdural hematoma. He had an electroencephalogram which showed features of moderate encephalopathy, but no seizures or epileptiform activity. He eventually required intubation for airway protection.
Case 2: Cryptococcal Meningitis
A male patient in his sixties with a history of lumbar disc herniation and spinal stimulator placement in 2021, hypothyroidism, and norm calcemic hyperparathyroidism presented after a fall while gardening and was noticed to have anisocoria. Over the month preceding presentation, he reported progressive lower extremity weakness, headaches, retro-orbital pain, light-headedness, and blurry vision. He was previously seen in the emergency department for these symptoms, along with chest pain, and was discharged with plans for outpatient cardiac workup. Subsequently, he started having cognitive issues, including new difficulties with basic daily activities. He lived with his wife and had no history of exposure to birds or caves, although he vacationed in Kentucky, Ohio, and Pennsylvania over the prior year. In terms of surgical history, he had multiple lumbar microdiscectomies at L4-5 with eventual L4-5 posterior lumbar interbody fusion. This was complicated by persistent dysesthesias in his left foot, prompting dorsal column stimulator placement at T8 in 2021. He also had carpal tunnel release surgery one month prior to presentation.
His neurological exam was notable for significantly impaired attention and concentration. He was noted to have increased reflexes, graded as 2 plus in both upper and lower extremities symmetrically. He was also noted to have anisocoria and the absence of a pupillary constriction to light in both eyes, prompting an Ophthalmology evaluation. He underwent a lumbar puncture, and Infectious Disease was consulted based on his cerebrospinal fluid culture findings, below.
Investigations
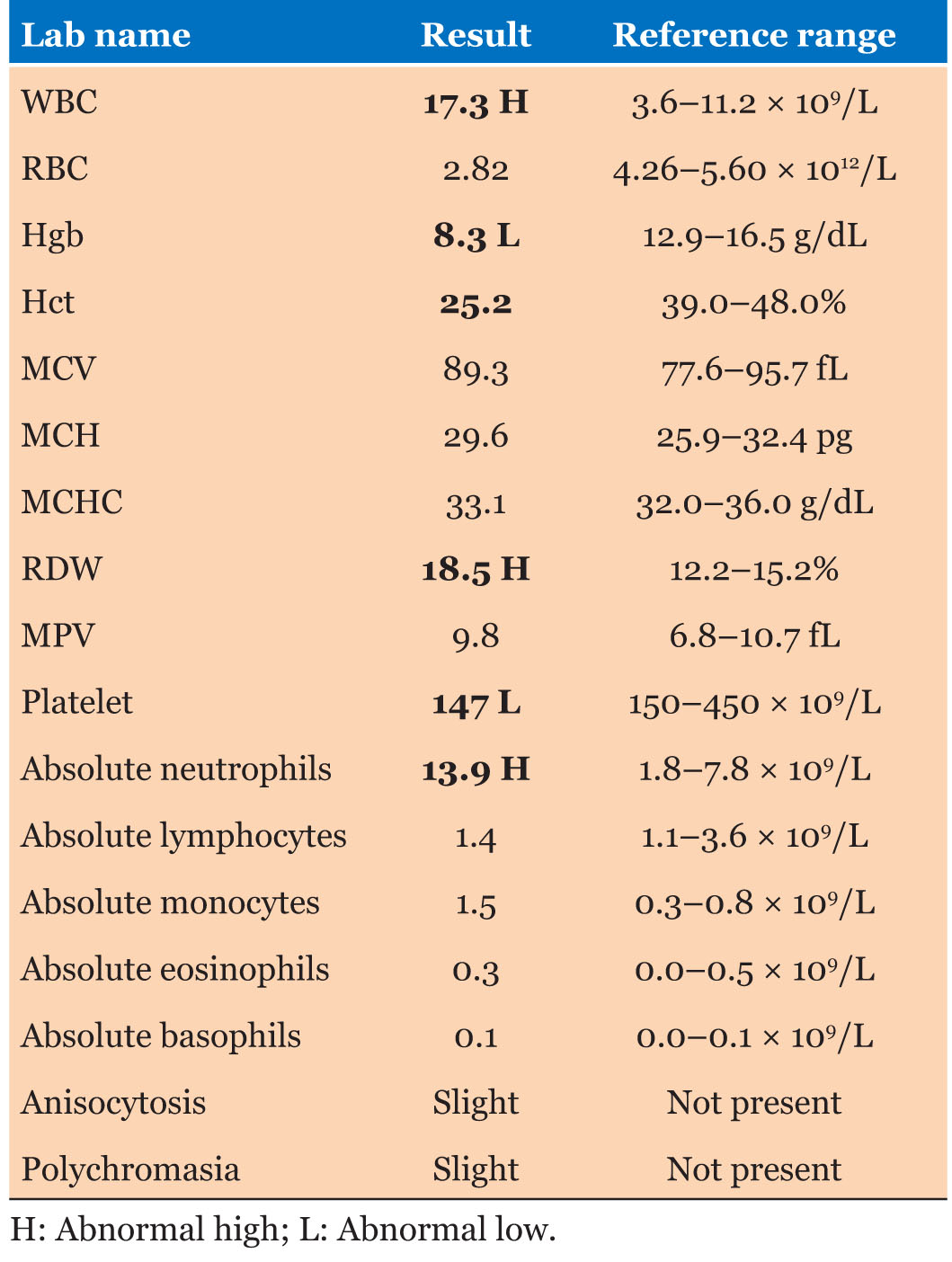
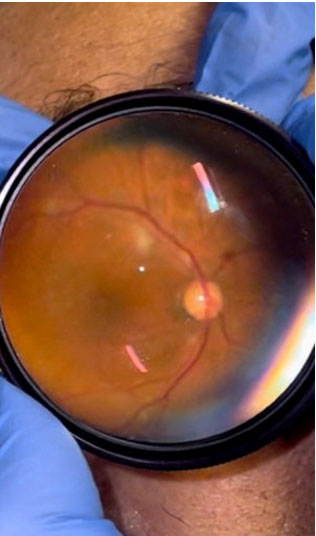
Case 1: Initial workup was notable for a negative HIV test, a leukocytosis with neutrophilic predominance (Table 1), and negative blood cultures from peripheral draws and a central line. However, repeat blood peripheral cultures yielded Cryptococcus neoformans. The serum cryptococcal antigen was also positive, with a titer of 1:640. A lumbar puncture was not clinically feasible due to the presence of a rightward midline shift and the associated risk of uncal herniation, limiting central nervous system (CNS) assessment. The image of the chest did not indicate infection, and echocardiography showed no valvular vegetations. An ophthalmology examination revealed multiple white creamy lesions deep to the retina in the left eye, consistent with fungal endophthalmitis (Figure 1).
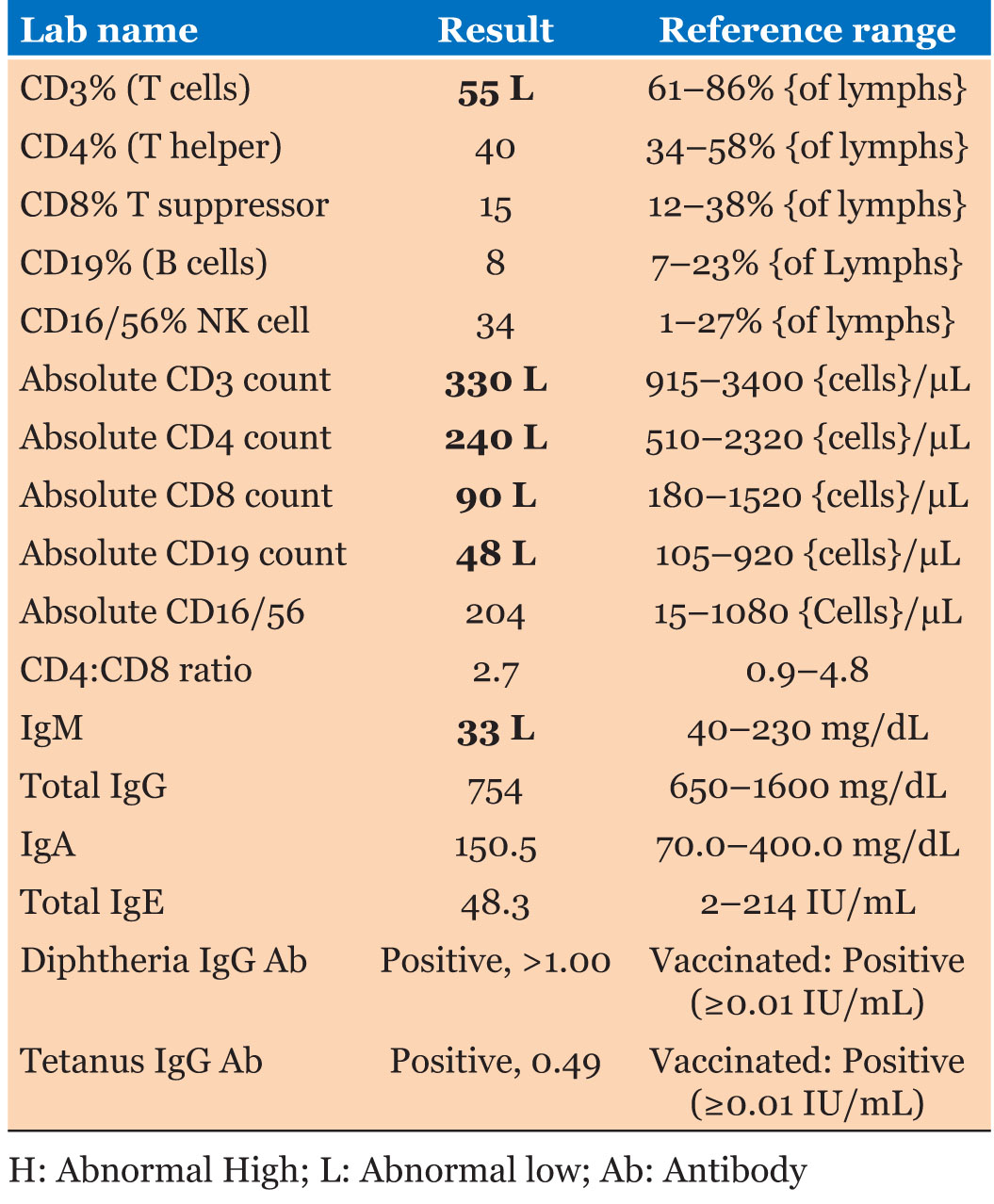
Case 2: Initial laboratory tests revealed a normal total white blood cell count, normal kidney and liver function, and negative HIV and rapid plasma reagin (RPR) tests. A lumbar puncture was obtained with an opening pressure of 16 cm H2O, a leukocytic pleocytosis (52 cells/μL, reference ≤5 μL), elevated protein (89 mg/dL, reference 19–65 mg/dL), and hypoglycorrhachia (31 mg/dL, reference 48–79 mg/dL). A cerebrospinal fluid (CSF) culture was positive for Cryptococcus neoformans. A CSF cryptococcal antigen was positive with a titer of 1:1280 and a serum cryptococcal antigen was also positive with a titer of 1:5120. A complete blood count (CBC) with differential was within normal limits except for persistent lymphopenia throughout admission (range of 0.4–0.9, reference 1.1–3.6 × 109/L). His absolute CD4, CD8, CD3, and CD19 cell counts were below normal range, while immunoglobulin levels were within normal to low normal ranges (Table 2). Tetanus and diphtheria antibodies returned at protective levels. Per chart review, the patient was lymphopenic as early as 2019, with absolute lymphocyte count 0.8 × 109/L (reference 1.5–5.0 × 109/L).
Differential Diagnosis
Case 1—differential diagnosis for persistent fevers in intensive care unit (ICU)
- Invasive fungal infection, as patient was febrile on broad spectrum antibiotics
- Central nervous system infection, secondary to bilateral hygromas and subdural hematoma as nidus
- Syphilis vasculitis
- Silent aspiration events
- Hospital acquired pathogen via tracheostomy tube
- Acalculous cholecystitis versus Pancreatitis
- Pressure ulcer infection
- Possible drug related fever reaction
Case 2—differential:
- Cryptococcal meningoencephalitis
- Bacterial meningoencephalitis
- CNS Syphilis infection
- CNS viral infection: arbovirus, varicella zoster, toxoplasmosis, Epstein–Barr virus (EBV), cytomegalovirus (CMV), adenovirus, enterovirus
- CNS malignancy
Treatment
Case 1: The patient was initiated on liposomal intravenous (IV) Amphotericin B 4 mg/kg daily and flucytosine 25 mg/kg four times a day for disseminated cryptococcal infection.
Case 2: The patient was started on induction treatment for cryptococcal meningitis with liposomal IV amphotericin B 4 mg/kg daily and flucytosine 25 mg/kg four times a day.
Outcome and Follow-up
Case 1: Due to the progression of the hematoma on imaging and worsening mental status attributed to worsening intracranial hemorrhage, he was transitioned to comfort care. The patient is currently at home with hospice.
Case 2: The patient had steady improvement in cognition with cryptococcal-directed therapy. A repeat lumbar puncture showed an opening pressure of 7 cm H2O, persistent leukocytic pleocytosis (63 cells/μL, reference ≤5/μL), elevated protein (67 mg/dL, reference 19–65 mg/dL), and normal glucose level (48 mg/dL, reference 48–79 mg/dL), all improved compared to initial lumbar puncture. Cerebrospinal fluid culture finalized without growth. The patient was transitioned to maintenance therapy of fluconazole 800 mg daily, discharged, and has since continued to improve at home, approaching his baseline.
Immunology was consulted for assistance in working up underlying immunological factors. His pneumococcal antibody levels were protective (>1.3 mcg/mL) for 15/23 serotypes. However, the patient received the pneumococcal 20-valent conjugate vaccine two months prior to admission and thus interpretation of these values is limited. Lymphocyte proliferation in response to mitogens found that on day 0 lymphocyte viability at 74%, just barely below the threshold of 75%, but T and B cell proliferation responses to mitogens phytohemagglutinin (PHA) and pokeweed mitogen (PWM) were normal. A mutation panel was sent to evaluate for genetic causes of primary immunodeficiency, but was unrevealing. Following this workup, a repeat lymphocyte subsets count was repeated 6 weeks after his initial presentation, and showed that his CD4 count was 462, while his CD3 count was 682—both still lower than normal range, but improved from prior. His transient lymphopenia suggests temporary immune dysregulation, predisposing to opportunistic infection despite the lack of an overt immunodeficiency.
Discussion
Cryptococcus spp. are environmental basidiomycetous fungi [3] first identified by Busse and Buschke in 1894 [4] A notable increase in invasive cryptococcal infections has been observed since the HIV pandemic [5], with Cryptococcus neoformans and Cryptococcus gattii being the primary species involved in cryptococcal disease. C. neoformans primarily comprises serotypes A and D, while C. gattii includes serotypes B and C [5]. Due to widespread vaccination against Streptococcus spp. and H. flu and increased use of immunosuppressive therapy, Cryptococcus spp. Have become an increasingly common cause of CNS infection worldwide, including in patients without a known immunocompromising condition at time of diagnosis. These patients have lower rates of positive CSF cultures and are more likely to clear cultures after two weeks of therapy.
Cryptococcus spp. possess several virulence factors, with the most significant being a thick polysaccharide capsule that aids in evading phagocytosis by the host immune system [5]. Cryptococcus neoformans exhibits unique pathogenicity, notably its ability to survive at 37°C and secrete diphenol oxidase, which facilitates melanin production. Melanin not only enhances survival in the environment but also renders melanized C. neoformans more resistant to degradation by host defenses, including cell wall-degrading enzymes [6].
Diphenol oxidase functions as an antioxidant, enabling extended survival within host cells by consuming superoxide ions, although it primarily protects against extracellular enzymes rather than intracellular ones. This capability is a major virulence factor, contributing to the organism’s pathogenicity [7]. Both C. neoformans and C. gattii have a propensity to infect the central nervous system, especially in patients with impaired cell-mediated immunity. In addition to neurological infections, Cryptococcus can affect the lungs, skin, bones, joints, and eyes [8]. The antiphagocytic capabilities of Cryptococcus allow it to evade phagocytosis by macrophages, employing a survival strategy akin to that seen in environmental amoebas [9]. This phenomenon, often referred to as the “Trojan horse” mechanism, facilitates dissemination through the bloodstream and the crossing of the blood-brain barrier, leading to invasion in microcapillaries [10]. Cryptococcus gattii, primarily found in tropical regions, has been associated with infections in immunocompetent hosts, whereas C. neoformans predominantly causes disease in those with impaired immune systems, such as people with HIV [11].
As Cryptococcus infections become more prevalent overall, diverse clinical presentations must be kept in mind when evaluating for the pathogen. For the patient in case 1 with NASH cirrhosis, there is a known association of susceptibility to cryptococcus in patients with cirrhosis [12]. Research suggests immune dysfunction in the setting of cirrhosis—specifically impaired cell-mediated immunity and surveillance—may be important in driving susceptibility to Cryptococcus, especially spread to less common organ systems [13]. Cirrhosis is associated with a 5.3 fold higher rate of extrapulmonary dissemination [14] and was likely a risk factor for our patient. While the cause of the patient’s subdural hematoma was thought to be due to recent falls, we do note the inability to definitively rule out a CNS infection with a lumbar puncture.
Meanwhile, there have been increasing numbers of invasive C. neoformans infections found in seemingly immunocompetent individuals, prompting further investigation into these atypical presentations. The patient from case 2 was initially suspected to have idiopathic CD4 lymphopenia, due to the history of persistent lymphopenia in the absence of exposure to immunomodulating medications, viral infections, or malignancy. Other case reports have been published documenting the connection between idiopathic CD4 lymphopenia and disseminated cryptococcus infections [15]. However, as noted above, repeat lab work six weeks later showed improvement in all lymphocyte lines, and his absolute CD4 count of 462 cells/μL put him above the threshold (less than 300) required for diagnosis of idiopathic CD4 lymphopenia [16]. The underlying etiology of his years-long lymphopenia, as well as the cause of its resolution, remains unclear, but his case emphasizes the importance of considering Cryptococcal infections in patients without overt immunocompromising conditions.
Conclusion
These cases underscore that disseminated cryptococcosis can occur in patients without classical immunosuppression, particularly those with subtle immune compromise. Early recognition and prompt antifungal therapy are critical for favorable outcomes.
REFERENCES
1.
Pappas PG. Cryptococcal infections in non-HIV-infected patients. Trans Am Clin Climatol Assoc 2013;124:61–79.
[Pubmed]

2.
Pappas PG, Perfect JR, Cloud GA, Larsen RA, Pankey GA, Lancaster DJ, et al. Cryptococcosis in human immunodeficiency virus-negative patients in the era of effective azole therapy. Clin Infect Dis 2001;33(5):690–9. [CrossRef]
[Pubmed]
3.
Alanio A. Dormancy in Cryptococcus neoformans: 60 years of accumulating evidence. J Clin Invest 2020;130(7):3353–60. [CrossRef]
[Pubmed]
4.
May RC, Stone NRH, Wiesner DL, Bicanic T, Nielsen K. Cryptococcus: From environmental saprophyte to global pathogen. Nat Rev Microbiol 2016;14(2):106–17. [CrossRef]
[Pubmed]
5.
Srikanta D, Santiago-Tirado FH, Doering TL. Cryptococcus neoformans: Historical curiosity to modern pathogen. Yeast 2014;31(2):47–60. [CrossRef]
[Pubmed]
6.
Nosanchuk JD, Casadevall A. Impact of melanin on microbial virulence and clinical resistance to antimicrobial compounds. Antimicrob Agents Chemother 2006;50(11):3519–28. [CrossRef]
[Pubmed]
7.
Jacobson ES, Jenkins ND, Todd JM. Relationship between superoxide dismutase and melanin in a pathogenic fungus. Infect Immun 1994;62(9):4085–6. [CrossRef]
[Pubmed]
8.
Maziarz EK, Perfect JR. Cryptococcosis. Infect Dis Clin North Am 2016;30(1):179–206. [CrossRef]
[Pubmed]
9.
Alvarez M, Casadevall A. Phagosome extrusion and host-cell survival after Cryptococcus neoformans phagocytosis by macrophages. Curr Biol 2006;16(21):2161–5. [CrossRef]
[Pubmed]
10.
Coelho C, Bocca AL, Casadevall A. The intracellular life of Cryptococcus neoformans. Annu Rev Pathol 2014;9:219–38. [CrossRef]
[Pubmed]
11.
Kwon-Chung KJ, Varma A. Do major species concepts support one, two or more species within Cryptococcus neoformans? FEMS Yeast Res 2006;6(4):574–87. [CrossRef]
[Pubmed]
12.
Singh N, Sifri CD, Silveira FP, Miller R, Gregg KS, Huprikar S, et al. Cryptococcosis in patients with cirrhosis of the liver and posttransplant outcomes. Transplantation 2015;99(10):2132–41. [CrossRef]
[Pubmed]
13.
Cheng JH, Yip CW, Jiang YK, Zhou LH, Que CX, Luo Y, et al. Clinical predictors impacting cryptococcal dissemination and poor outcome in patients with cirrhosis. Open Forum Infect Dis 2021;8(7):ofab296. [CrossRef]
[Pubmed]
14.
Baddley JW, Perfect JR, Oster RA, Larsen RA, Pankey GA, Henderson H, et al. Pulmonary cryptococcosis in patients without HIV infection: Factors associated with disseminated disease. Eur J Clin Microbiol Infect Dis 2008;27(10):937–43. [CrossRef]
[Pubmed]
15.
Sim BNH, Hui LY, Krishnan D, Joseph JP. Idiopathic CD4 lymphopenia in a case of disseminated cryptococcosis with brain, vertebral spine and reproductive organ involvement. Clin Med (Lond) 2019;19(2):133–4. [CrossRef]
[Pubmed]
16.
Lisco A, Ortega-Villa AM, Mystakelis H, Anderson MV, Mateja A, Laidlaw E, et al. Reappraisal of idiopathic CD4 lymphocytopenia at 30 years. N Engl J Med 2023;388(18):1680–91. [CrossRef]
[Pubmed]
SUPPORTING INFORMATION
Author Contributions
Salma Gayed - Conception of the work, Design of the work, Acquisition of data, Analysis of data, Drafting the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Stephen Schworer - Conception of the work, Design of the work, Acquisition of data, Analysis of data, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Elgin Yalin - Conception of the work, Design of the work, Acquisition of data, Analysis of data, Drafting the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Joseph Stromberg - Acquisition of data, Analysis of data, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Michael Herce - Conception of the work, Design of the work, Acquisition of data, Analysis of data, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Guaranter of SubmissionThe corresponding author is the guarantor of submission.
Source of SupportNone
Consent StatementWritten informed consent was obtained from the patient for publication of this article.
Data AvailabilityAll relevant data are within the paper and its Supporting Information files.
Conflict of InterestAuthors declare no conflict of interest.
Copyright© 2026 Salma Gayed et al. This article is distributed under the terms of Creative Commons Attribution License which permits unrestricted use, distribution and reproduction in any medium provided the original author(s) and original publisher are properly credited. Please see the copyright policy on the journal website for more information.