|
Case Report
Follmann balanitis as an atypical form of primary cutaneous syphilis
1 Al Wattan Medical Group, Riyadh 11461, Saudi Arabia
2 Dermatology and Andrology Department, Suez Faculty of Medicine, Suez University, Suez 41552, Egypt
3 Dermatology Department at Sheikh Jaber Al-Ahmad Al-Sabah Hospital, Kuwait
Address correspondence to:
Ahmed Bakr Elazab
Suez Faculty of Medicine, El-zahra district, Suez 41552,
Egypt
Message to Corresponding Author
Article ID: 100020Z16AE2026
Access full text article on other devices

Access PDF of article on other devices


How to cite this article
Bakr Elazab A, Ibrahim Ali A, Mohamed Eldisoky I. Follmann balanitis as an atypical form of primary cutaneous syphilis. J Case Rep Images Infect Dis 2026;9(1):9–12.ABSTRACT
Introduction: Follmann balanitis is a rare and atypical manifestation of primary syphilis, characterized by erosive, inflammatory lesions of the glans penis that can mimic other infectious or inflammatory causes of balanitis. Due to its unusual clinical appearance, misdiagnosis or delayed diagnosis is common, emphasizing the importance of maintaining a high index of suspicion in sexually active individuals.
Case Report: A 33-year-old male presented with a painful erythematous plaque with erosions over the glans penis, persisting for 20 days. The lesion appeared eight days following unprotected oral and vaginal heterosexual intercourse. There was no history of new medication use, drug intake, systemic symptoms, or previous similar episodes. Physical examination revealed a large, well-demarcated erosive erythematous plaque involving the glans and extending to the foreskin, with no associated regional lymphadenopathy or other cutaneous lesions. Based on the sexual history, a comprehensive screening for sexually transmitted infections was performed. Swabs from the erosive lesions were negative for bacterial and fungal cultures, and herpes simplex virus polymerase chain reaction (HSV PCR) results were also negative. Serological testing demonstrated a positive Treponema pallidum hemagglutination assay (TPHA 1/320) and a positive rapid plasma reagin (RPR 1/32), confirming the diagnosis of primary syphilis presenting as Follmann balanitis. The patient was treated with a single intramuscular dose of 2.4 million international units of benzathine penicillin G, resulting in significant clinical improvement within two weeks. Rapid plasma reagin (RPR) titer dropped to fourfolds within three months.
Conclusion: This case underscores the importance of considering syphilis in the differential diagnosis of atypical erosive balanitis. Prompt serological testing and appropriate antibiotic therapy are essential for achieving rapid resolution and preventing disease progression or transmission.
Keywords: Erosive balanitis, Follmann balanitis, Primary syphilis, Sexually transmitted infections, Treponema pallidum
Introduction
Syphilis is a sexually transmitted infection caused by Treponema pallidum (TP), and its prevalence has increased dramatically worldwide in recent years [1]. Given the increased incidence, more attention should be paid to the atypical presentations of primary syphilis in order to prevent further serious complications [2]. We present a case of Follmann balanitis in a middle-aged male patient, which is a rare and atypical presentation of primary syphilis.
Case Report
A 33-year-old male patient visited our clinic with a painful erythematous plaque with some erosions on the gland penis that had been present for 20 days. There was no history of new medications being introduced, and the patient denied any drug use. The patient reported that the lesion appeared eight days after having unprotected oral and vaginal heterosexual intercourse. A large, erosive, well-defined erythematous plaque over the glans had spread to the foreskin (Figure 1).
No skin lesions or enlarged lymph nodes were present. Herpes simplex virus (HSV) polymerase chain reaction (PCR), bacterial and fungal cultures of swabs from erosive lesions, and serologic tests for human immunodeficiency virus (HIV) and syphilis were among the screening tests for sexually transmitted infections (STIs) that were conducted based on the patient’s sexual history. All the investigation results were negative except for positive Treponema pallidum hemagglutination assay (TPHA) 1/320 and positive rapid plasma regain test (RPR) 1/32. According to the investigation results, we excluded the diagnosis of herpes simplex, mycological infection and bacterial infection, and the diagnosis of Follmann balanitis was made. There was no history of previous syphilitic infection. The patient was treated with a single intramuscular injection of 2.4 million international units of benzathine penicillin, with great improvement achieved within two weeks (Figure 2). After three months, the RPR titer dropped fourfold.


Discussion
Sexually transmitted infections like syphilis are brought on by T. pallidum infections. Sexual contact is the most common way for transmission to occur. However, studies have shown that nonsexual ways, like mouth-to-mouth transmission of previously chewed food, can also result in syphilis infection [3]. The clinical presentation of syphilis varies widely, despite the fact that it is generally described as progressing through primary, secondary, latent, and tertiary stages. After an incubation period of roughly 21 days, the primary infection typically manifests as a painless genital chancre and inguinal lymphadenopathy [2]. Balanitis refers to the inflammation of the glans caused by a variety of factors. Several pathogens contribute to the development of infectious balanitis, including fungal, bacterial, anaerobic, parasitic, and viral agents. Eugene Follmann first described syphilitic balanitis, and the condition was later named after him [4].
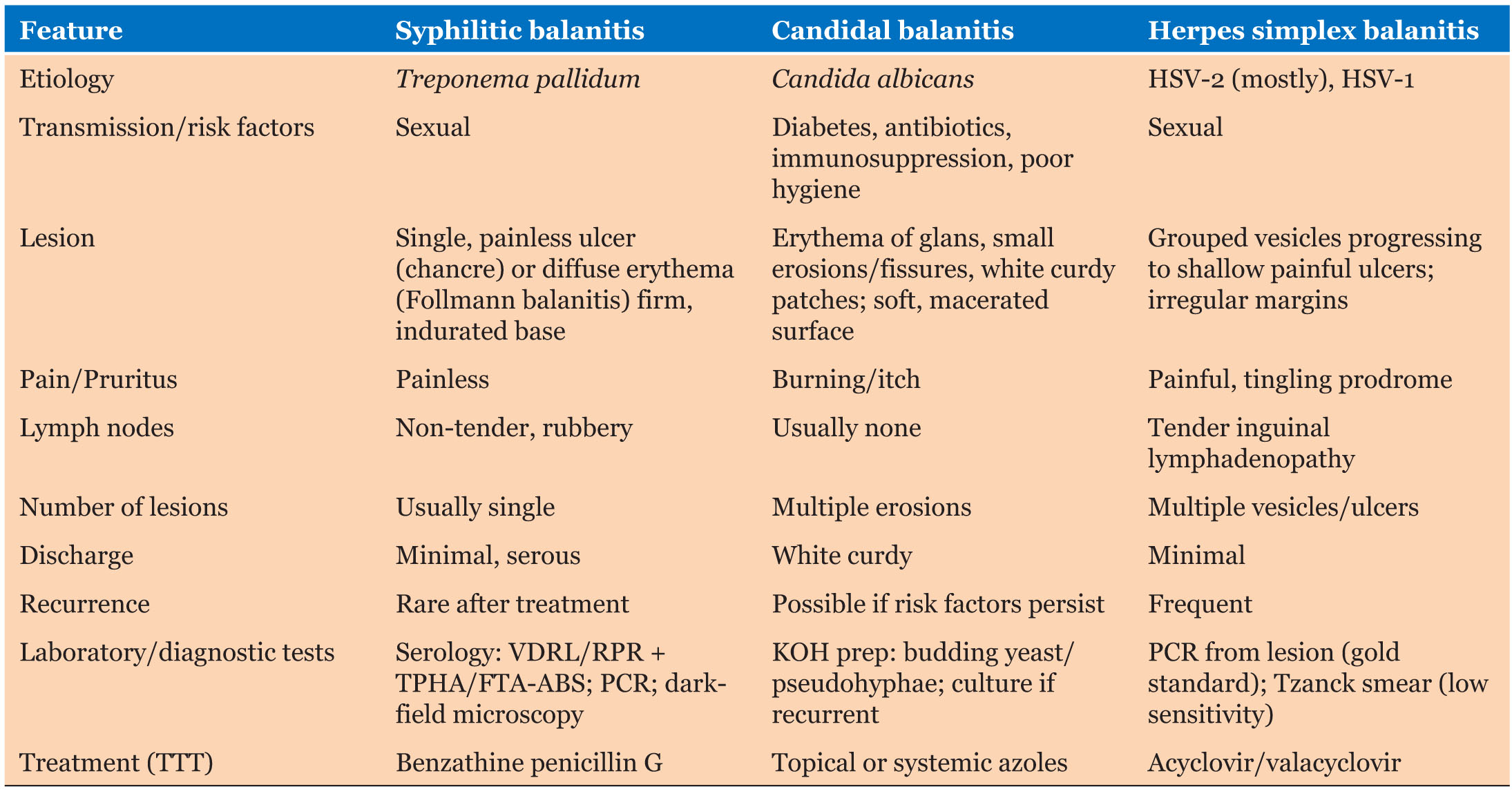
We present a case of Follmann’s syphilitic balanitis, which may be a rare manifestation of primary syphilis. This observation, in our opinion, deserves special attention. As the condition is frequently misdiagnosed as another cause of balanitis, such as herpes simplex or Candida albicans. Follmann balanitis, unlike the “classic” syphilitic chancre, is large, superficial, and painful.
Another drawback is the results of serological testing; Hembert et al. found that 36% of patients with primary syphilis had both negative treponemal and nontreponemal tests, and 60% of patients had a negative nontreponemal test [5]. Salle et al. also reported a case of Follmann balanitis with a negative Venereal Disease Research Laboratory (VDRL) and TPHA [1]. Therefore, even though polymerase chain reaction is not yet commonly used in clinical practice, it is the most effective direct diagnostic assay for detecting Treponema pallidum [1] (Table 1).
Conclusion
Follmann balanitis is an atypical, rare form of primary syphilis that is frequently misdiagnosed as other causes of balanitis. With the increasing incidence of syphilis infection in recent years, clinicians should be aware of the condition and suspect T. pallidum infection in cases presenting with balanitis, especially with a suggestive sexual history. Early management of syphilis can prevent subsequent health care utilization and long-term sequelae.
REFERENCES
1.
Salle R, Cavelier-Balloy B, Duong TA, Dauendorffer JN. Syphilic balanitis of Follman presenting as a painful erosive balanitis with negative treponemal serology. Indian J Dermatol Venereol Leprol 2025:1–2. [CrossRef]
[Pubmed]

2.
Patel M, Gioia P, Jha P. Follmann balanitis: An unusual case of syphilis. WMJ 2024;123(2):144–6.
[Pubmed]
3.
Long FQ, Wang QQ, Jiang J, Zhang JP, Shang SX. Acquired secondary syphilis in preschool children by nonsexual close contact. Sex Transm Dis 2012;39(8):588–90. [CrossRef]
[Pubmed]
4.
Oanţă A, Irimie M. Syphilitic balanitis of Follmann. Int J Dermatol 2014;53(7):830–1. [CrossRef]
[Pubmed]
5.
Hembert R, Salle R, Grange PA, Ollagnier G, Benhaddou N, Heller U, et al. Evaluation of the usefulness of routine molecular biology for the diagnosis of primary syphilis by assessing the serological status of patients with PCR-confirmed syphilitic ulcers. J Eur Acad Dermatol Venereol 2024;38(7):e590–2. [CrossRef]
[Pubmed]
SUPPORTING INFORMATION
Author Contributions
Ahmed Bakr Elazab - Conception of the work, Design of the work, Acquisition of data, Analysis of data, Drafting the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Ahmed Ibrahim - Acquisition of data, Analysis of data, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Islam Mohamed Eldisoky - Acquisition of data, Analysis of data, Drafting the work, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Guaranter of SubmissionThe corresponding author is the guarantor of submission.
Source of SupportNone
Consent StatementWritten informed consent was obtained from the patient for publication of this article.
Data AvailabilityAll relevant data are within the paper and its Supporting Information files.
Conflict of InterestAuthors declare no conflict of interest.
Copyright© 2026 Ahmed Bakr Elazab et al. This article is distributed under the terms of Creative Commons Attribution License which permits unrestricted use, distribution and reproduction in any medium provided the original author(s) and original publisher are properly credited. Please see the copyright policy on the journal website for more information.